
The Scale We’re Not Using (But Could Be)
While casually hanging out in a light blue paper gown, waiting for the dermatologist’s knock, I noticed two posters on the wall.
Well, I didn’t so much notice them as they commanded my attention.
These double-hung, window sized posters were—full color and impossible to ignore. They showed all the common lesions and disorders of the skin including skin cancer—and which ones, if left untreated, could kill you.
They were equal parts fascinating and unsettling. I tried to look away (seriously, it was a bit gnarly), then reminded myself, “Good grief, you’re at the dermatologist’s office being proactive with the largest organ in your body (a full 20 square feet of surface area!). Now’s not the time to be squeamish.”
So I pushed past my discomfort, got up, and took a closer look. Skin cancer is no longer a word without additional context for me. The posters made sure of that. The reality is, I see my dermatologist once a year. I’m with my skin 365 days a year—I know it better than anyone.
It’s helpful to know what I’m looking for.
But that poster got me thinking…
Where is the illustrative poster normalizing how our bodies shift and change over time—including as we approach end-of-life? This is the mind of a death doula at work!

I’m envisioning a holistic tool. One that captures the essence at 1,000 ft, it doesn’t need to be granular, as we’ve all lived different lives and that means different health journeys.
You and I, we come from a long line of dead people who lived to varying ages and died (suddenly, or over time) from a smorgasbord of things. We’ve all observed how people slow down in different ways. Gravity and living takes their toll–our engine has seen some miles. We’ve also seen the impact illnesses have—with and without treatment.
The more I keep my head on a swivel and stay curious, the more I recognize (and honor) shared patterns. We talk about our “original equipment” and how it creaks and squeaks—but often in an apologetic way, like it’s something to be ashamed of that we are getting older and are no longer thirty-something.
The reality? We all have only so many heartbeats. And even if we were all born on the same day, countless variables influence our final odometer reading.
Maybe that’s the argument for “no poster.”
But that hasn’t stopped us from creating helpful, supportive guideposts for the front end of life—What to Expect When You’re Expecting, What to Expect in the First Year, and so on, plenty of variables exist with each birth as well.
Isn’t it about time we gave equal airtime (or wall space) to what to expect as we approach our later chapters—not just when we’re actively dying?
What we pay attention to
Of course, we do have tools to track our health over time. From our first breath, our weight is captured—likely before diaper number one is even in place. As children grow, vital stats are collected, charted, and discussed. As adults, it’s expected that we monitor bloodwork and blood pressure—normal, high, low—and yes, we still slip off our shoes to get the most accurate weight (a nod to those diaper-free beginnings).
Any single data point only tells us so much. But over time, reviewed together, they form a bigger picture.
It’s finding our own place on the scale that’s useful, from our individual vantage point.
We’ve learned to track these numbers. We understand where we land in relation to others. And with that information, we make adjustments—course corrections—and promise to revisit later down the road.
Ideally, we maintain an ongoing conversation with our bodies.
But a healthy body is more than cholesterol levels and blood pressure readings…right?
Then there’s the “secret” score!
At my annual physical this year, I asked about a couple numbers in my bloodwork. My provider wasn’t concerned. Yes, they were outside the range—but overall, I had scored “X” based on my total health picture.
Wait…what?
I have a secret score?
My initial excitement quickly faded. I didn’t get a copy. I have no idea how it’s calculated. All I know is it was “good.” (Or maybe: “okay, passable, not dying yet.”)
That mystery is what bothers me.
As a death doula, I’m always looking for ways to help us have richer, more complete conversations about our whole selves—with each other and with our medical teams. Especially in a world where many of us see multiple specialists each year, and visits increasingly shift from prevention to managing chronic conditions.
Afterall, there will come a time when what I eat or drink won’t positively shift the numbers. Exercise won’t move the needle the same way. Medications will stop improving—or even stalling—the inevitable. My body won’t be trying to optimize anymore. Instead it will follow its natural course, perhaps with a few comorbidities along for the ride.
My time will eventually be up. The extended warranty will expire. I will have met—or exceeded—my expected mileage (that will always remain an illusive number) and I will die.
And just like the beginning of life, it would be helpful to acknowledge, recognize and honor the wind-down stages. Can we get a scale for that, please?
Better yet—can we put it on a poster in our primary care offices and in a pamphlet we can take home?
A reality check on aging
Today, people around the world are living longer—and in greater numbers than ever before. But aging doesn’t follow a neat, predictable path. As the World Health Organization puts it:
“These changes are neither linear nor consistent, and they are only loosely associated with a person’s age in years.”
In other words—two people the same age can and will have different experiences with their bodies. And we know this because:
“At the biological level, aging results from the accumulation of molecular and cellular damage over time…leading to a gradual decrease in physical and mental capacity, a growing risk of disease and ultimately death.”
Still, we make talking about this part of living taboo—while simultaneously fueling an $85 billion anti-aging industry. So how can we ground ourselves in reality and start these conversations earlier, rather than when we turn 65 and our primary care provider has the “advance care planning” talk? Better yet, how can we support someone that is navigating the results of aging (and or disease) that is grabbing a lower (not always a slower) gear?
It turns out there is a scale we can use
I recently discovered the existence of a scale that is practical, holistic and begins with fully functioning (100%) to our final breath (0%).
It’s public. It’s widely used (worldwide) and it's called the PPS.
The PPS looks at five areas:
Ambulation
Activity & evidence of disease
Self-care
Intake (nutrition and hydration)
Conscious level
In other words: It grounds us in the five essential aspects of daily living and gives us a way to determine how our body is functioning overall.
Wondering where this handy-dandy scale has been hiding?
Palliative care and hospice professionals have been using it since the late 90’s. Its official name is the Palliative Performance Scale (PPS for short).
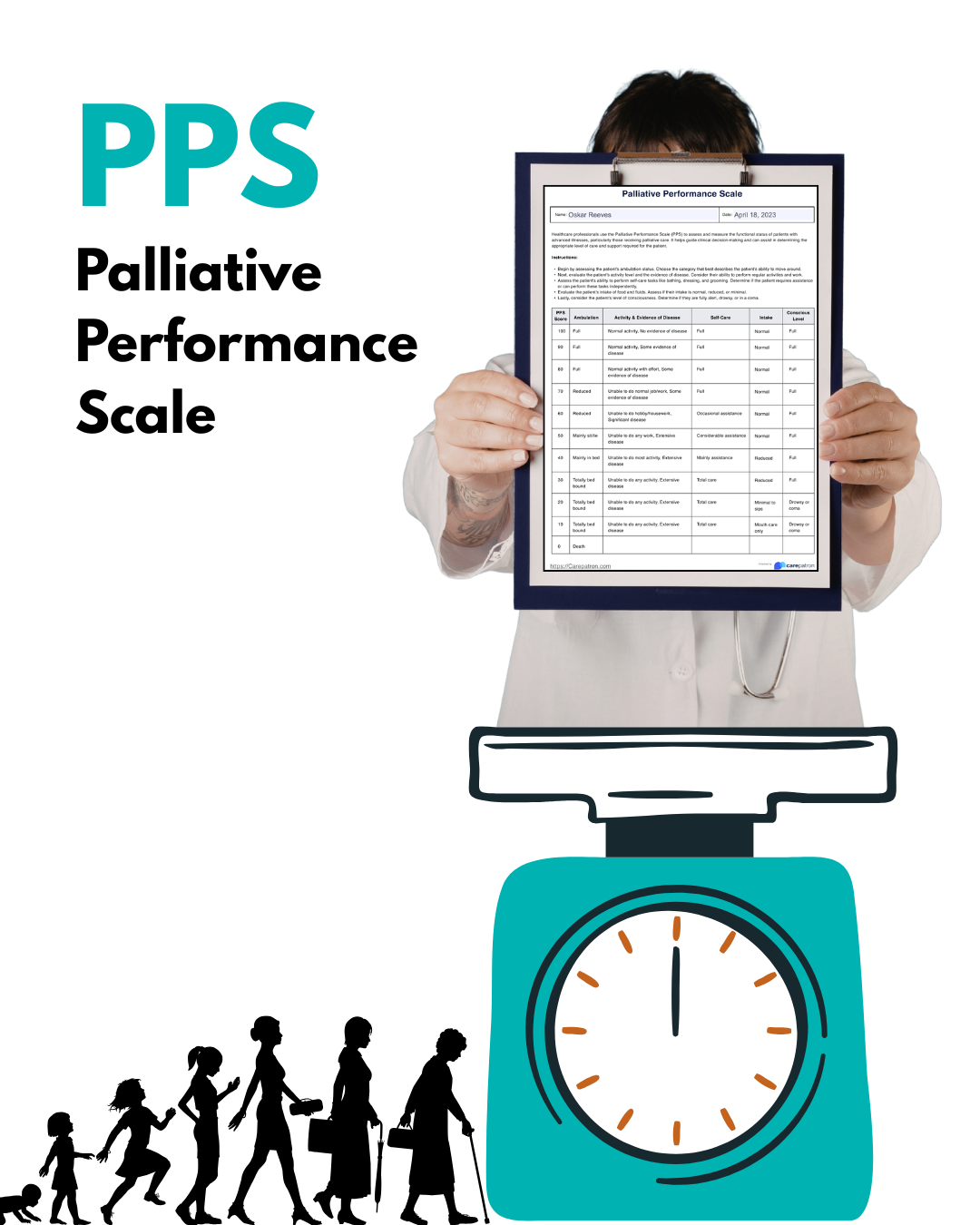
The PPS zooms out to about 100 ft. for a regular fly by, taking in the bigger picture you. And while developed for clinicians, you don’t need a medical degree to read it. The PPS is also one of the tools used to help determine hospice eligibility — another reason for us to familiarize ourselves with it given how often hospice is not offered as continuity of care, when it could be.
I propose we agree to use it “off label”!
What if we used the PPS like an annual skin self-check or personal health review?
What if we filled it out before appointments, brought it into conversations with our providers (they are already familiar with it), used it with our caregivers and family, and kept a copy of it on the fridge (more on that later). Not to predict anything. But to notice patterns and changes over time.
What if we used it when considering treatment options? Not as a rule or a limitation, but as a question: “If I go down this path…what might this look like on the PPS over time given where I am today? Or “Would this proposed treatment improve function? Maintain it? Reduce it? For how long?”
We use data for everything else. Why not here?
You and I are part of a movement to bring our eventual dying into conversations about our living encompassing both quality and quantity. The PPS feels like a missing piece—not because it predicts the future, but because it gives us language for the present and the future.
I’ve taken a few of these small steps with the PPS already.
For instance, I have a copy of the PPS on the side of my fridge—right next to family photos and various travel postcards. It’s my version of the dermatologist’s poster that is visible, shared and I can refer to it over time. Everyone visits the fridge after all.
Instead of waiting for a provider to hand us a score we can bring our own to the conversation with our health care support team.
And I’ve shared the PPS with my dad and my sister (who lives five minutes from him). I asked my dad if he’d be up for reviewing it and to let me know where he’d place himself.
His response? “70%.” A man of few words.
Now we have a shared baseline (by the way — I agree with his percentage) and common language along with a way to check in that doesn’t rely on guessing, but instead self awareness and observations. And when that number shifts—as we know it will–we already have meaningful and historical insight into what that new number represents. We now have a tool to help us discuss how best to support him at every % point along the way.
I don’t expect my dad to stay at 70%. There will be 60% days if they already don’t show up now and again. This isn’t about predicting decline, it’s about recognizing it as it naturally will happen—together with the understanding and respect for our bodies. Recognizing we have a life span and we don’t need to wait for someone else to assign us a number, we can bring that number to them to advocate for continuity of care where it matters most.
Afterall, that dermatologist’s poster didn’t tell me if I’d get skin cancer. It showed me what to look for—so I could act sooner if I needed and wanted to. The PPS does the same thing, and knowledge really does feel like power.
All this brings us to some SMALL STEPS to consider.
Do one or some of these for yourself or through the lens of a caregiver.
Look up the Palliative Performance Scale. Get familiar with it HERE . Download a copy and follow the instructions on how to use it.
Give yourself a score—for today This is a lens, not a verdict. After all you are with your body 365 days of the year, your observations matter.
Bring it into conversation: “Can we use something like this to track how things are going?” If you’re a caregiver, this is a great tool for you and your person to review together, compare notes and bring your questions to your medical providers.
Notice changes over time: Energy. Movement. Appetite. Engagement. Self-care. Bring those changes to conversations with your medical care team, your home care team and folks it would be important to have these conversations with that want to support you. We can better advocate for continuity of care when we are looking further down the road and have time to explore options based upon what matters most.