
What If We Do Nothing?
I’ve started asking a question in medical appointments that, without fail, garners a very specific facial expression—the one where you know the person is wondering if they heard you correctly.
And it seems to always buy me more time (bonus) with my healthcare professional, along with a lively discussion.
It sounds something like this: after I recap the treatment options (for my own clarity), I suggest they may have forgotten one (bold, I know!). I ask: “What if I do nothing?”
Not “do nothing” in the neglectful sense. Not “do nothing” because I don’t value medicine. Not “do nothing” because I’m giving up.
Rather, what happens if we also give equal consideration to the option that almost never gets discussed alongside the others? And, this is key, what if we also map that option in parallel—not just as a cul-de-sac turnoff at the first bend in the road, but as far as what is known about the treatments options being suggested?
What will my healthcare provider learn about me from that discussion? And what will I better understand about the road ahead?
Over the last several years, working with people navigating advancing frailty, serious illness, and end-of-life, I’ve noticed something. Most medical conversations are heavily weighted toward intervention. Toward fixing. Toward action.
And that makes sense. Medical professionals are trained to problem-solve. To repair what can be repaired, offer options and, hopefully, ease suffering as well.
But somewhere along the way, many of us forget we’re not simply a collection of body parts and diagnoses. We are more than that. We are whole people, and we are not our disease or ailment.
Treatment decisions impact our living—and frankly speaking those caring for us too. And when there is no known cure, these decisions become about extending life—our life.
Based on clinical trials and knowledge gained over time, expectations and impacts related to treatment options will be shared. But shouldn’t we also be discussing what foregoing treatment looks like for my whole self?
Because here’s what I’ve come to appreciate: we are provided a diagnosis and a treatment plan, but rarely a comparative roadmap with all the options.
Which is why I started what I jokingly refer to as my own longitudinal study. The constant in this study is me. My whole body. My whole self. The variables? Every healthcare professional I’ll encounter over the next two-three decades.
My guiding principle is simple: I have to bring my whole self into every medical appointment—not just the organ, disease, limb, or ailment of the day. And whenever treatment options are presented, I ask about the one that rarely gets equal airtime: doing nothing.
The question deserves a place in the exam room. And because it’s not often brought up, it’s preemptively discounted as a bona fide option to holistically and logistically consider alongside the exact same criteria when considering a treatment path.
One of the first times I practiced this approach was at my dentist’s office (have to start somewhere). I was there discussing the fate of the crown on tooth #32. It had already required multiple visits after refusing to stay seated, and the proposed solution was to start from scratch with an entirely new crown. (Note: this dentist was not the one that originally placed this crown, if you were wondering.)
Cost: $2,000 give or take.
My dentist explained his sole recommendation and paused, assuming we had reached the end of the conversation. But I remember responding:
“I don’t think you’ve given me all my options yet.”
That got his attention, and yes, I got the did I hear that correctly look too.
I explained that I also wanted to understand the health implications of doing nothing—short term and long term—given that the tooth already had a root canal, I didn’t have dental insurance, and I wanted to weigh all the realities before making a decision.
For a moment, things got a little awkward for both of us. Based on the dentist’s reaction, I suspected it was a situation he didn’t encounter often.
But once he understood (or actually accepted) what I was actually asking, he gave me a direct reply.
“You’ll probably be fine for a very long time. Maybe forever.”
And just like that, the conversation changed.
Not only did I leave with more information, but my dentist also left knowing a little bit more about me—not just tooth #32. He understood that finances mattered to me. That I wasn’t looking for a dental-book-perfect-fix simply because it existed. That I was trying to evaluate the treatment in the context of my whole life, whole body, and what that meant for future me.
That interaction clarified something important for me.
Too often, medical conversations happen in fragments. The cardiologist focuses on the heart. The orthopedist focuses on the joint. The oncologist focuses on the cancer. The neurologist focuses on the brain. And while each specialist may be excellent within their lane, the person living inside the body has to carry the cumulative impact of every recommendation.
And along with them, the medications. The appointments. The recovery periods. The caregiving needs. The financial burden. The transportation logistics. The side effects. The tradeoffs. The uncertainty. The time.
As we age and accumulate multiple conditions, this fragmentation is amplified, and communication becomes more complex and nuanced
As an end-of-life doula I supported an individual navigating Stage IV throat cancer who asked their oncology team for a bit more clarity around disease progression–given the length of time already spent with chemo. They wanted to make sure they were spending their time in ways that mattered most to them and better understand what “the end” might realistically look like (there were fears of suffering)—only to be told they didn’t need to worry because they had “plenty of time.”
That person died a month later.
I’ve also supported people navigating multiple serious illnesses and difficult treatment decisions. Sometimes there is a treatment path available for one condition—but pursuing it may do little to meaningfully change the outcome of another condition that’s more concerning, limiting, or ultimately more likely to shape how they live and die.
These aren’t simple decisions.
People often aren’t asking only: Can we treat this?
They’re also asking: What happens if we do? What happens if we don’t? Will this meaningfully improve my life? What am I gaining—and what am I spending to pursue it?
People want medical providers to explain—not just the treatment itself—but what life might realistically look like with and without it. Not simply, you’ll die sooner.
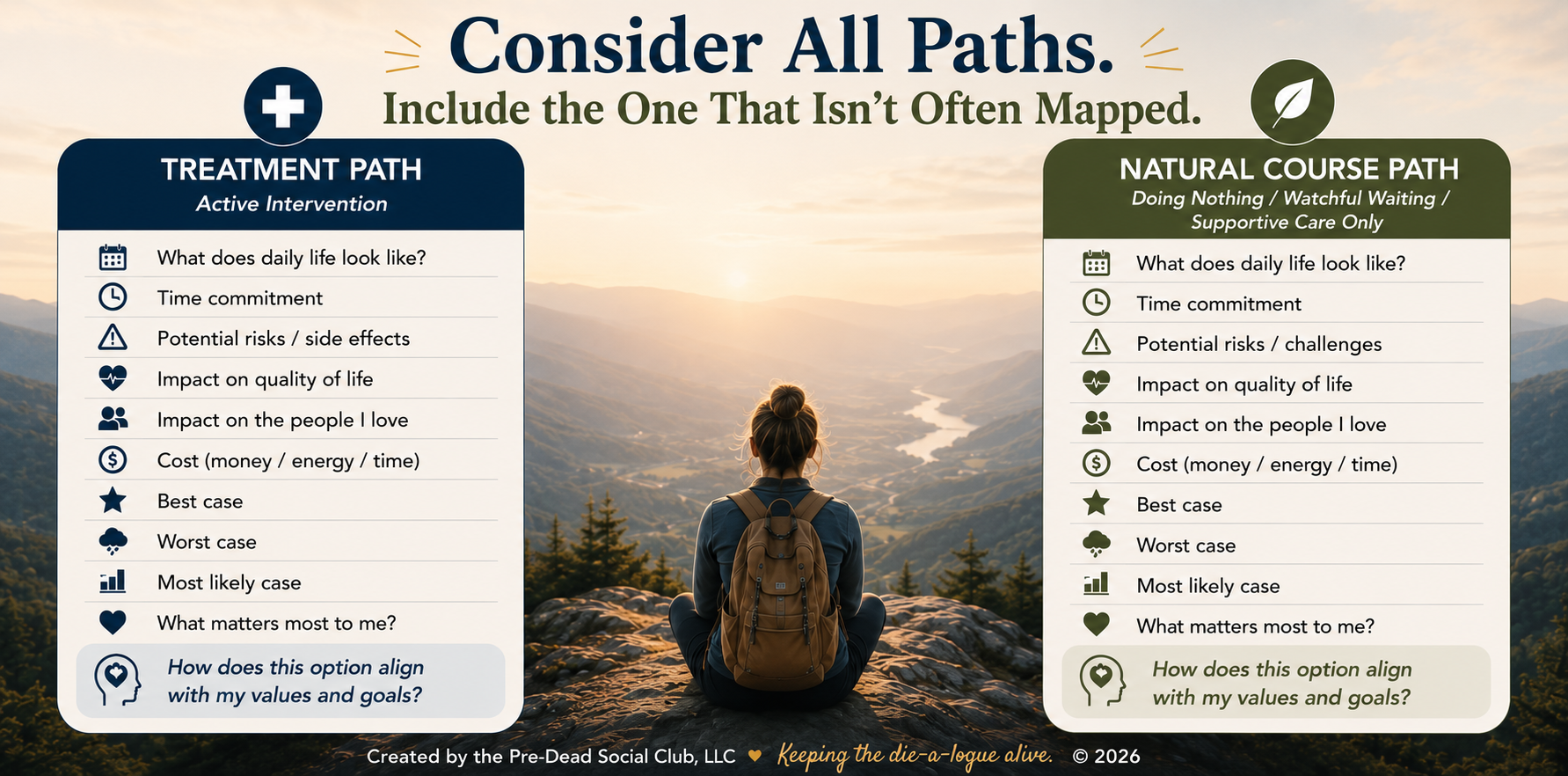
I’ve seen this time and time again. Patients are often offered a diagnosis and a treatment plan, but rarely an illness roadmap. The medical world knows a lot about many diseases, thus the treatment recommendations. So, let’s put that knowledge to use as best as possible with a side-by-side look using the same criteria:
What does the road look like with treatment “X” and without it? How might each path impact quality of life? Independence? Caregiving needs? Financial realities? The ability to remain at home? Time (this one is layered)? The amount of “good days” (according to who?) the treatment hopes to gain—let alone all the days spent pursuing the treatment path itself.
And yes, I say “days spent” intentionally because time is a currency. In the non-treatment model, we often talk about the number of days remaining. But when treatment is involved, we rarely add up how those days, weeks, or months will actually be spent. In bed? In appointments? Recovering? Traveling? Feeling well enough to enjoy the people and activities that matter most?
Let’s compare not just the number of days—but how they’re spent—side-by-side in relation to what matters most to the person living inside the body?
As a 60+ year old human, I recognize statistically I’ll likely face increasingly complex medical decisions in the decades ahead. That’s not pessimism. That’s simply being mortal.
I also know medicine (at least in the US) will continue offering more interventions, more devices, more procedures, more clinical trials, more possibilities. Some of those may absolutely improve or extend my life in meaningful ways—to me—based upon my metrics, not the medical system’s.
But I never want to confuse the existence of an available treatment with an automatic obligation to pursue it.
Which is why I’ll keep asking about the “do nothing” option.
That question is robust enough to open the doors to conversations that matter most—but often remain unspoken. Money. Fear. Exhaustion. Caregiving realities. Personal priorities. Acceptance. How someone defines quality of life. How they value their remaining time and the quality of it as they define it.
And it helps to illuminate the subtle, but important, difference between extending life and prolonging dying.
By putting the “do nothing” option on the table, you just might open the conversation your trusted medical provider wants to have, but doesn’t quite know how to start—and you made the first move. Yep, many are waiting for a sign from you to have this important discussion. Depending upon their perspectives, they may or may not see dying as a failure of medicine and they can’t read your mind either.
And no, “doing nothing” won’t always be the path, but sometimes it will. If we never examine it alongside the other options, then we aren’t fully informed for some of our most important decisions.
I’m not a professional researcher. But I do hold expertise in one area no medical professional can fully possess: I live inside this body. I know what makes my life feel like my life. And I’m gaining clarity on what tradeoffs are acceptable to me. I know what quality and quantity of life mean in my own lived experience.
Over the last two years, I found myself in a different version of “do nothing.” This time, I was between two trusted medical providers with very different approaches to the same symptoms. One I had known for over thirty-five years, the other newer to my care, but equally thoughtful and consultative.
What surprised me most was not simply that they disagreed, but how strongly they disagreed—especially after three years of pursuing a treatment path (we all agreed on) that had produced little to no improvement. Under the new treatment approach, I was getting pieces of my life back.
What unfolded wasn’t simply a disagreement about medicine. It was about two trusted professionals assessing risk, long-term outcomes, and quality of life through very different lenses. And there I was, sitting in the middle of it feeling like I had to defend feeling well to the doctor I’d known the longest.
It was unsettling.
At one point, the conversation turned toward life expectancy and risk. And for the first time, I heard myself clearly say out loud:
“Then maybe I’ll have fifteen really good years instead of twenty-five painful ones.”
That wasn’t me being reckless. It was me recognizing that quality and quantity of life are deeply personal calculations, and that I needed to articulate what that meant for me–today.
What felt especially important about that moment wasn’t that I changed anyone’s mind. It was that I crossed an internal threshold. I articulated—clearly and unapologetically—what mattered most to me. Based on my metrics, not the medical provider’s or the medical system.
I suspect this situation was practice for future crossroads still to come. It struck me that someday this could look like navigating cancer treatment options, where there will likely be strong opinions about what I “should” do not only from medical professionals, but from my family and friends.
We gain agency that we often lack in communicating with our medical providers, in asking the “do nothing” question. After all we are the ones who live with the consequences, tradeoffs, and outcomes of our medical decisions. Clarity shared today with trusted medical professionals, family, and friends better enables us to advocate for the care that matters most—with our whole body in mind.
So I encourage everyone, when the opportunity arises, to go ahead and ask the unexpected question:
“What happens if I do nothing?”
You might be surprised by the answer.
All this brings us to some SMALL STEPS to consider.
Get Familiar with Some Roadmaps: The folks at Waiting Room Revolution have developed some Illness Roadmaps for Alzheimer's Disease, ALS, Chronic Obstructive Pulmonary Disease and Ovarian Cancer.
They also offer a blank roadmap template that can be used to help chart any other illness. Check them out here.
Check out our Resources tab where you’ll find our FREE tool that gets the wheels turning to help frame decisions for medical decisions today.
We all exist somewhere between thriving and dying. At some point we’ll be asked to make weighty decisions (assuming death doesn’t come suddenly) as they relate to our health and how that affects quality and quantity of life.